Overcoming clinical diagnostic testing barriers in precision medicine
The improved patient outcomes that precision medicine can provide depend on the accurate identification of patients eligible for treatment. However, multiple barriers in the clinical diagnostic testing landscape work against the seamless integration of diagnostic testing into the treatment pathway. This can block patient access to tests and more so to precision medicines.
These hurdles can be grouped into 6 key barriers: Clinical Utility, Sample Availability, Test Availability, Test Quality, Test Turnaround Time, and Test Reimbursement.
Clinical Utility: Awareness of the clinical utility of the biomarker in an indication is key. Physician awareness of biomarker tests is vital as treating physicians initiate the testing sequence by ordering the tests. It’s also crucial that labs are aware of the utility so that they can offer the appropriate test. A lag in adoption of tests often ensues due to a lack of awareness of the clinical utility of new biomarkers and associated therapies. It is therefore important to consider; is the test recommended in guidelines; is it on test menus and order forms; are KOLs recommending the test; are labs reporting the actionability of this biomarker in their report forms? The establishment of clinical utility is often more of a hurdle in indications where the biomarker is novel, or where predictive biomarker testing is new to the patient journey.
Sample Availability: it’s important that there is enough sample available for the test. Sample availability is more of a barrier in indications where biopsies are small and/or difficult to obtain and where there are many actionable biomarkers, such as NSCLC.
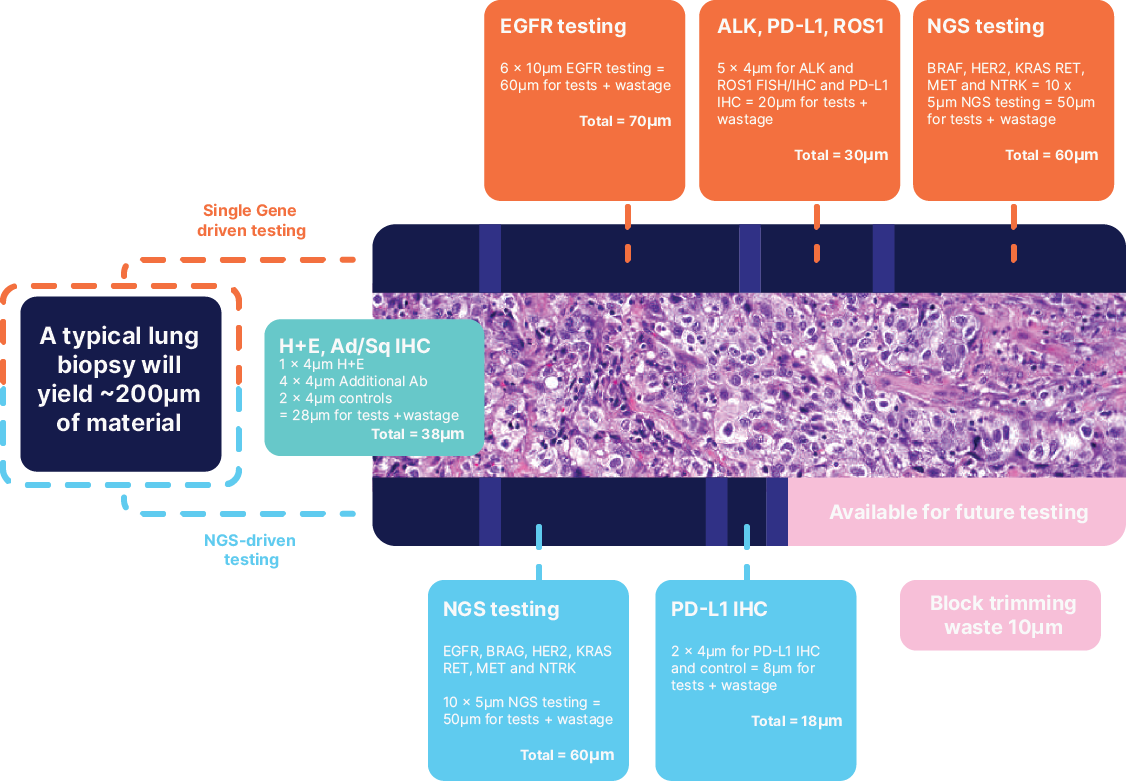
This is where tissue sparing methodologies such as NGS have become incredibly important, as an NGS approach, for the same biomarkers consume less tissue leaving some material for any future tests. This is also where LBx becomes useful, as it bypasses the issues we see with sample availability.
Testing Availability: The availability of testing is key to adoption, but equally important is the availability of the test in labs that physicians prefer and trust. It is important for pharma to understand the test availability landscape as it pertains to the methodologies preferred, the platforms used for testing, the preferred assays, and whether they are commercial assays or LDTs. The regulatory status, the ontology it can detect, and the sample type utilised should also be considered among many others. This information is important to support pharma to implement the most effective diagnostic strategy through the identification of the highest priority laboratories for engagement, understanding of the key stakeholders and lab types and through the support CDx partnership decisions.
Test Quality: False negatives and positives have a major impact on patient outcomes by misguiding treatment decisions and denying patient therapy that can be efficacious, or recommending one that could cause unnecessary harm due to side effects. The accuracy and the reliability of the CDx test is important so that physicians have confidence in prescribing the associated product. To analyse this barrier in the landscape it is important to explore if and how labs are accredited and to which standards. Secondly, assessing EQA participation to ensure labs are participating in relevant quality assurance programs. The participation in EQA is important for all labs testing biomarkers, but especially those utilising lab developed tests which have a higher chance of variation of quality.

Test Turnaround Time (TAT): The time it takes for a test to be completed and the results to be reported to the requesting physician is crucial in the delivery of appropriate treatment. Many factors can impact TAT; often dictated by methodology, e.g. NGS takes many more days than IHC to report results. Sample shipping and storage requirements can impact transit time, resulting in suboptimal analyte quality, repeat testing or request for new sample, thereby extending turnaround time. Send-out testing to another lab can also add a few days to the overall TAT . Additionally, labs may batch samples and reduce test frequency to enable cost efficiencies, resulting in additional delays.
Test Reimbursement: Sufficient reimbursement is key to driving test adoption by labs and physicians. Many factors can influence reimbursement decisions and values. Even if a test is reimbursed, the reimbursement value may not be sufficient to cover a lab’s cost. Where reimbursement is sub-optimal, labs will often look to develop their own Laboratory Developed Test's (LDT’s) which can result in higher variations in quality. Where reimbursement is very strained, labs may withdraw the offering of the test entirely, thus reducing overall test availability. Reimbursement systems vary between markets, and some require significant patient co-payments. This could increase socio-economic healthcare disparities whereby only patients who can afford the test can access it.